Partners in Care
Gillette Children's Partners in Care Blog provides up to date stories from our providers that focus on the innovation and research that underlies the care we provide our patients.


Pediatric Brain Injury: When to Refer to Rehab
June 22, 2026Pediatric patients who sustain an acquired brain injury (ABI) can experience varying degrees of functional deficits. An inpatient setting allows for close monitoring of progress and allows changes to be made to treatment recommendations in real time.
Read More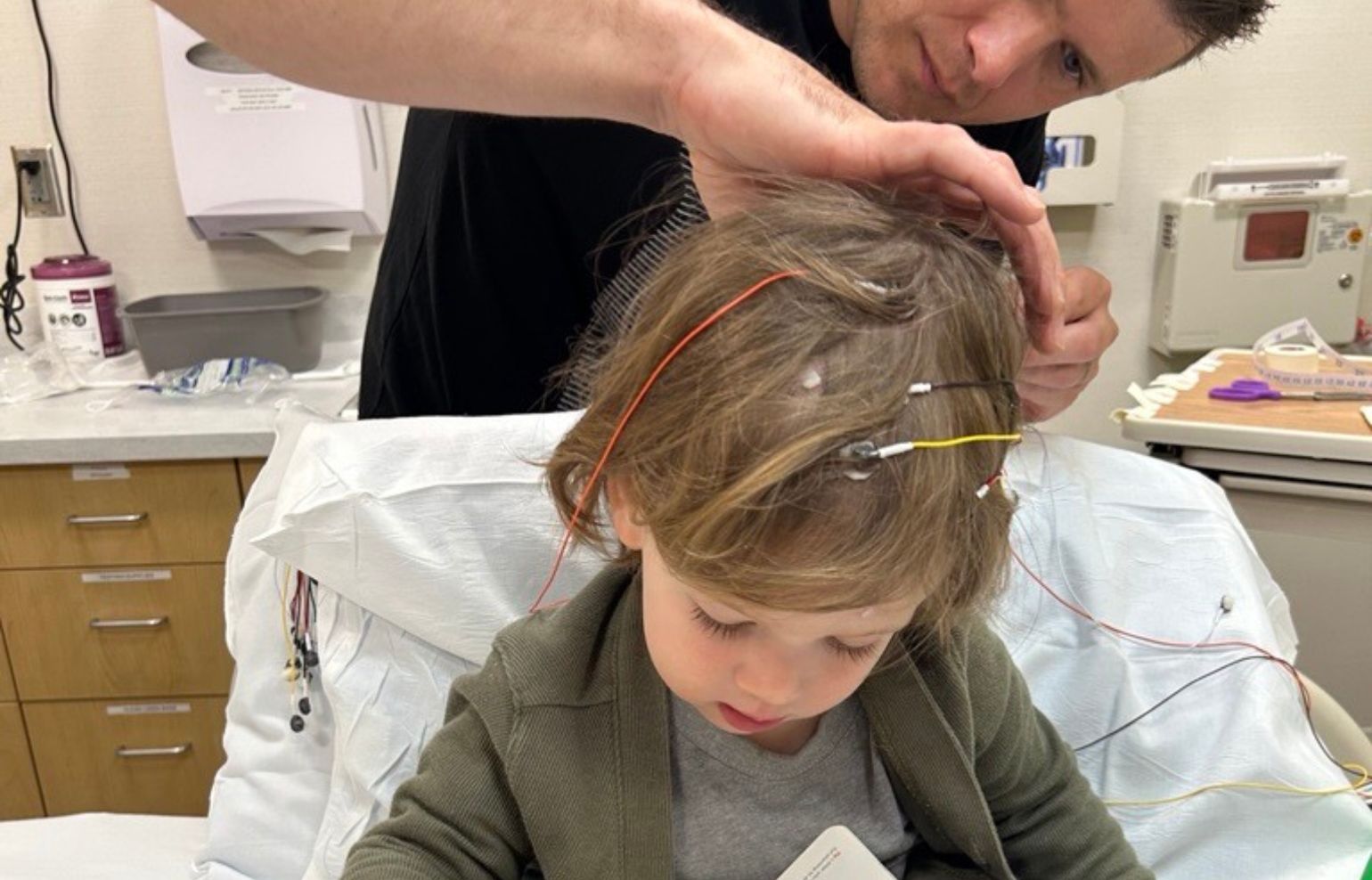
Seizure Evaluation Clinic: Easy Access to Neurology Experts
May 11, 2026The Seizure Evaluation Clinic is an entry point to expert pediatric care at Gillette Children’s with excellent access.
Read More
Early Diagnosis and Intervention for Cerebral Palsy
March 2, 2026Early diagnosis and intervention for cerebral palsy are critical for better treatment outcomes.
Read MoreJoin Our Partners in Care Community!
Subscribe to Partners in Care Journal, a newsletter for medical professionals.
Subscribe Today
Hip Care at Gillette Helps Illyana Become a Stronger Softball Player
November 4, 2025When Illyana was 12, she began to feel pain in her back and hips. That prompted her mother to schedule an appointment with Gillette Children’s.
Read More
Hip Dysplasia Referral Guide
November 4, 2025Gillette Children’s offers comprehensive hip preservation care for adolescents and young adults.
Read More
Advancing Cranial Remolding Therapy
November 4, 2025Gillette Children’s has seen positive outcomes in treating positional cranial deformities since the introduction of the Talee cranial remolding orthosis.
Read More
Gillette Research Shows Periarticular Injections Improve Mobility and Decrease Length of Stay After Hip Preservation Surgery
November 4, 2025 Read More
Preventing Adult Hip Arthritis in Adolescence
November 4, 2025 Read More
Comprehensive Care and Empowerment for Children Who Have Limb Loss or Limb Differences
October 3, 2025Gillette Children’s has one of the nation’s highest concentrations of pediatric orthopedic surgeons — and the latest technology specifically designed to care for children who have limb differences.
Read More
Pediatric to Adult Healthcare Transition Initiative Expands
October 2, 2025Gillette's Pediatric to Adult Healthcare Transition has expanded to the Gillette Children’s Down Syndrome Clinic, and plans are in place to launch within the Complex Care Clinic by Fall 2025.
Read More
Partnerships Strengthen Gillette’s Down Syndrome Clinic Care
September 26, 2025A partnership with the Down Syndrome Association of Minnesota (DSAMn) as well as strong collaboration with other programs at Gillette Children’s makes the Gillette Down Syndrome Clinic stand out.
Read More
Deep Brain Stimulation for Complex Movement Disorders
August 25, 2025A deep brain stimulation implant gives Hazel more control over her movement.
Read MoreHealth Library
Find education related to your condition, procedure, care at home, and more.
Search Health LibraryResearch
Gillette Research aims to improve treatment options for children who have disabilities.
Explore Gillette ResearchNews
From innovations to innovators, Gillette Children’s shares our news as leaders in specialty care and research.
News Releases