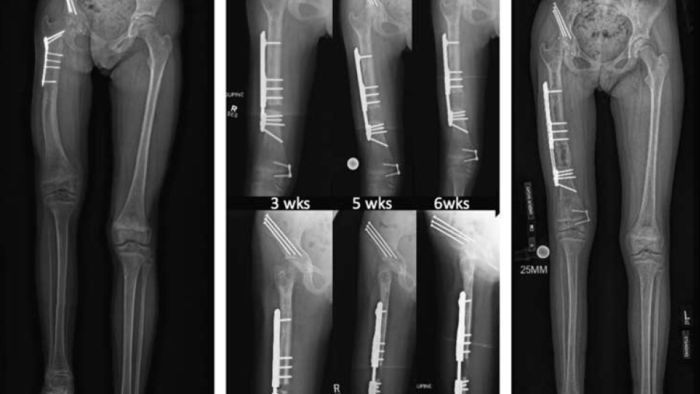
The latest limb lengthening study out of Gillette Children’s reports an innovative technology for the limb lengthening of femurs in small children. In the paper “Motorized Plate Lengthening of the Femur in Children: A Preliminary Report,” published in the Journal of Pediatric Orthopaedics, pediatric orthopedic surgeons Mark Dahl, MD, and Andrew Georgiadis, MD, prospectively collected data on a new limb lengthening implant starting in the fall of 2020 and into the early part of 2021.
Seven patients ages 2–9 received femoral lengthening surgery with a magnetic lengthening plate. “Because the implant is new, our goal was to be very rigorous in our documentation of outcomes, including details of their lengthening, radiographic outcomes, and complications to present the public with a good idea of its true utility,” says Dr. Dahl.
This research touches on a difficult aspect of limb lengthening treatment in young children with smaller bones. Small bones present a challenge because they still have open growth plates and anatomically may not be able to support an implant that goes inside the bone until a child’s pre-adolescent or adolescent years. Currently, most literature represents external fixation as the best choice for lengthening small bones. Dr. Dahl at Gillette Children’s has worked towards an alternative treatment paradigm for years.
“We were the first to publish about using an ‘inside of the bone nail’ outside of the bone, which is an off-label use that has been successful,” Dr. Georgiadis says. “We employ that method sometimes, but it’s not as good as an implant specifically designed to be outside the bone.” The current study evaluates just such an implant, one that goes inside the body but outside of the bone, intending to be safer for smaller bones in younger kids.
Successes and Difficulties of Treatment
In the new study, the team had two main conclusions. First, they found this kind of technology where a plate can distract and lengthen a small bone appears to be viable. Secondly, all seven young children had successful lengthening of the femur and experienced the same rate of complications and difficulties as other ways of lengthening, including external fixators. There are some complications unique to congenital limb quality compared to a child born with the normal limb who then developed a limb lengthening quality because of injury or infection. Dr. Dahl explains, “If you have a congenital limb lengthening quality, we can take away some of those burdens with better implants, but the implants don’t change the underlying diagnosis or some of the underlying difficulties that come with surgical lengthening.”
“The study itself is, I think, scrupulously open about the successes and difficulties in treating these patients,” Dr. Georgiadis says. Future research in this subspecialty is forthcoming. “We have a number of active projects in surgical lengthening of both acquired and congenital limb discrepancies, including some technical ways to do both corrective osteotomy and limb lengthening at the same site, which is very sparsely reported on,” Dr. Georgiadis says. “We’re excited to add to that body of work.”
Gillette Children’s is a referral center for complex limb differences. Led by Dr. Dahl, who has been performing limb length surgeries for more than 35 years, the limb lengthening and reconstruction team at Gillette is recognized both nationally and internationally.
Two Lengthening Technologies
Doctors have been performing limb lengthening for more than 100 years, but the techniques have changed significantly even in the last 15 years. One of the most common new treatment options is limb lengthening with implants that go inside the body and are lengthened using a handheld device.
Limb Lengthening via Implant
The lengthening implant is placed, and one or two weeks post-surgery, the patient's family initiates the lengthening process themselves at home. An external device with a magnet inside is placed on the limb. The family uses the device to telescope and lengthen the leg slowly over weeks, often 6 to 8 times per day, with each lengthening episode lasting about 20 seconds. “The lengthening process is unique in that a surgery happens, but the treatment is really done by the family at home,” Dr. Georgiadis explains. “From there, the family checks in with us on a weekly basis so we can clinically assess the lengthening site radiographically and adjust the lengthening rate and rhythm as needed. We routinely check in with patients who live out of state during a virtual visit using digital radiographs.” Though implants for limb lengthening have come a long way, for young children with smaller bones, external fixation is still a common treatment avenue.
Limb Lengthening via External Fixator
An external fixator is an apparatus with carbon fiber rings, stainless steel pins, and wires that traverse the skin. Using this device to lengthen a femur, results in a significant amount of pin care, including cleaning all the sites where pins and wires enter the child’s leg. As the leg is lengthened, those pins and wires can cause discomfort and scarring. While external fixators are necessary for specific situations, there is a move away from these devices for most limb-lengthening surgeries.
“External fixators have unique complications both physically and psychologically for a child and family,” Dr. Georgiadis says. “We want to decrease the burden on the family undergoing limb lengthening as much as possible, so we try to use these internal methods whenever we can.”
Join Our Partners in Care Community!
Subscribe to Partners in Care Journal, a newsletter for medical professionals.
Subscribe Today